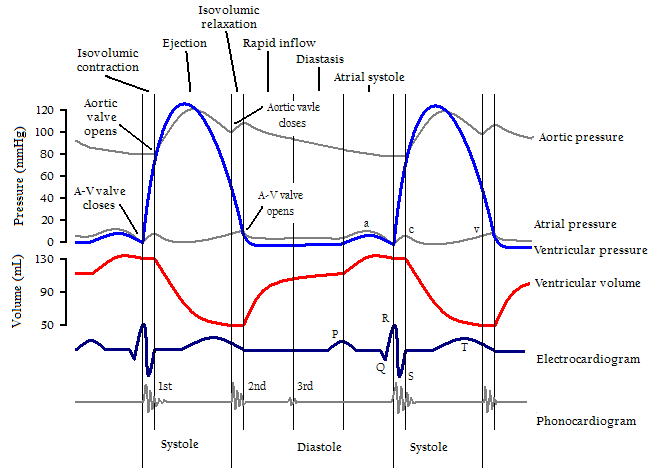
filling occurs during diastole, which has 4 phases: (1) isovolumic relaxation; (2) rapid filling phase; (3) slow filling, or diastasis; and (4) final filling during atrial systole (atrial kick.)
Cardiac Cycle
- Isovolumic relaxation – this phase occurs after the aortic valve closes and the mitral valve is still closed. LV relaxation is energy dependent, requiring ATP. Calcium first dissociates from Troponin C, allowing actin to dissociate from myosin. Calcium is then taken back into the sarcoplasmic reticulum by SERCA-2. There are also elastic recoiling forces of proteins such as titin that aid in relaxation.
- Rapid filling – this begins after left atrial pressure has exceeded the pressure within the LV and the mitral valve opens, allowing passive blood flow into the LV. This phase contributes the largest volume during filling.
- Slow filling – occurs as the LV pressure approaches the L atrial pressure. It contributes 5% of total diastolic volume. The L atrium acts as a conduit during this phase, allowing venous return to flow through the LA into the LV. LV pressures can decrease to sub-atmospheric pressures, causing a diastolic suction phenomenon.
- Atrial systole – Last 15% (on average) of LV volume is delivered as the atria contract. This is more important with high heart rates and LV hypertrophy.
LV filling can become impaired and lead to heart failure with preserved ejection fraction (diastolic dysfunction.) Impaired LV relaxation decreases rapid filling so more of the LVEDV must be derived from atrial systole. Reduced LV compliance causes increased LVEDP that can result in pulmonary edema.
LV compliance is dependent on myocardial characteristics (volume independent, such as hypertrophy) and chamber characteristics (volume dependent.) Causes of impaired LV filling include myocardial ischemia, which inhibits the amount of ATP available for isovolumic relaxation. LV hypertrophy from HTN, or chronic LVOT obstruction such as AS, is accompanied by increased fibrosis of the LV, decreasing the viscoelastic recoil properties of the heart.

Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.