Key Points
- Maximum allowable blood loss (MABL) is calculated using the patient’s estimated blood volume and hematocrit.
- Estimating intraoperative blood loss and calculating MABL can help prevent under-resuscitation and unnecessary blood administration.
Introduction
- Numerous studies have shown that blood transfusions have risks, including transfusion-associated circulatory overload, transfusion-related immunomodulation, and transfusion-related acute lung injury.1
- Preoperative anemia is an independent risk factor for poor perioperative outcomes.2 Anemia decreases oxygen-carrying capacity and oxygen delivery to end organs. When oxygen requirement exceeds oxygen delivery, tissue ischemia and end-organ damage can ensue. Since oxygen delivery depends on cardiac output and arterial oxygen content, patients with decreased cardiac output or hemoglobin concentration are at an increased risk of tissue ischemia, particularly in the setting of increased metabolic demand.
- Estimating MABL aids the anesthesiologist in deciding when blood administration may be necessary, in the context of the patient’s hemodynamics, surgical procedure, rate of ongoing blood loss, and underlying patient comorbidities.
Maximum Allowable Blood Loss (MABL) Calculation
MABL
=
EBV
⋅
(
HCTi
−
HCTf
)
HCTi
MABL = maximum allowable blood loss (in mL)
EBV = estimated blood volume (in mL/kg) (Table 1)
HCTi = initial preoperative hematocrit (in %)
HCTf = final hematocrit after blood loss (in %)
HCTf is the transfusion threshold that is determined by patient-specific factors.
| Age | |
| Premature infants | |
| Term newborns | |
| Infants less than 1 year | |
| 1 – 12 years | |
| 12 – 18 years | |
| Adult males | |
| Adult females | |
| Adults with a BMI of 30 | |
| Adults with a BMI of 40 | |
| Adults with a BMI of 50 | |
| Adults with a BMI of 60 |
Table 1. Estimate blood volumes for different age groups and sexes.3,4
Clinical Use
Preoperative Planning
- MABL should be calculated prior to every anesthetic where blood loss may be significant depending on the type of surgery, the patient’s bleeding tendencies, and whether the patient’s hematocrit is close to the transfusion threshold.
- MABL calculation is particularly important when caring for neonates and small children where small volumes of blood loss can still be clinically significant.
- MABL should be employed as a part of comprehensive patient blood management to optimize the patient’s blood health. Allogenic transfusions may be reduced by optimizing the patient’s preoperative hemoglobin, using intraoperative cell salvage, or administering antifibrinolytic therapy in appropriate patients and surgical procedures. Additionally, appropriate management of preoperative anticoagulation, including cessation timing and reversal of anticoagulation, is a necessary step in minimizing blood loss.
- MABL can also be used to guide the preparation and administration of blood products.
Intraoperative Management
- Surgical blood loss should be continually assessed and several methods to estimate surgical blood loss have been proposed.5
- Visual estimation of blood loss in sponges and suction canisters is the most commonly used method. Unfortunately, it is not accurate. Blood loss estimates for fully saturated surgical sponges are listed below (Figure 1).6,7
- 4 x 4 cm surgical gauze-10 mL
- Ray-techs-20 mL
- Pediatric surgical sponge-50 mL
- Large 30 x 30 cm surgical sponge-100 mL

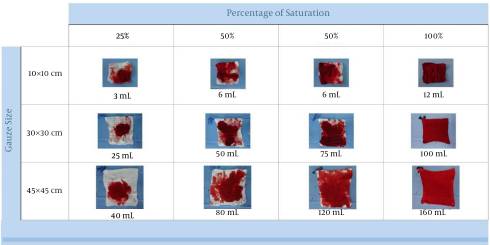
Figure 1. Visual guide for estimating blood loss. Source: Algadiem AE, et al. Blood loss estimation using gauze visual analogue. Trauma Mon. 2016.6 CC BY NC 4.0.
2. Gravimetric method: Blood loss is deduced by weighing the surgical material contaminated with blood and subtracting their dry weight. This method uses the conversion of 1g = 1 mL of blood.
3. Direct measurement of blood loss such as placing calibrated collection bags placed under obstetric patients; this method is not very commonly used.
4. Mathematical formulas to calculate blood loss (Moore formula, Nadler’s formula, etc.)
5. Colorimetric blood loss estimation: A smartphone application Triton™ (Gauss Surgical Inc, Los Altos, CA) takes photographs of used surgical gauze and canisters and uses feature extraction technology to calculate the hemoglobin mass and estimate the blood loss.
A recent meta-analysis showed the highest correlation with the colorimetric method. Both the visual estimation and the gravimetric method showed a high degree of bias.9
- Blood loss should initially be replaced with crystalloids to maintain euvolemia.
- Blood transfusion should be considered when surgical blood loss exceeds MABL, taking into consideration the patient’s hemodynamic status and the response to the blood loss.
- After fluid resuscitation, the patient’s hematocrit should be confirmed, when possible, prior to initiating a transfusion.
References
- Abdallah R, Rai H, Panch SR. Transfusion reactions and adverse events. Clin Lab Med. 2021; 41(4): 669-96. PubMed
- Hare GMT, Mazer CD. Anemia: Perioperative risk and treatment opportunity. Anesthesiology. 2021;135(3):520-30. PubMed
- Riley AA, Arakawa Y, Worley S, et al. Circulating blood volumes: A review of measurement techniques and a meta-analysis in children. ASAIO Journal. 2010;56(3): 260-4. PubMed
- Lemmens H, Bernstein D, Brodsky J. Estimating blood volume in obese and morbidly obese patients. Obes Surg. 2006; 16(6): 773-6. PubMed
- Gerdessen L, Meybohm P, Choorapoikayil S, et al. Comparison of common perioperative blood loss estimation techniques: a systematic review and meta-analysis. J Clin Monit Comput. 2021;35(2): 245-58. PubMed
- Algadiem AE, Aleisa AA, Alsubaie HI, et al. Blood loss estimation using gauze visual analogue. Trauma Mon. 2016; 21(2): e34131. PubMed
- Sharashchandra KV, Shivaraj SP. Intraoperative allowable blood loss: Estimation made easy. MedPulse International Journal of Anesthesiology. 2020; 14(1): 27-31. Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.