Key Points
- The physiologic effects of each patient position are exaggerated in an anesthetized patient since the compensatory mechanisms may be inhibited by the anesthetic.
- Positioning the patient is a shared responsibility among the anesthesiologist, surgeon or proceduralist, and nurse in the operating room.
Introduction
- Different patient positions may be required to provide access for different surgeries and procedures. Each position will impact the patient physiology and these can be exaggerated in an anesthetized patient since the compensatory mechanisms may be inhibited by the anesthetic.1,2
- Positioning the patient is a shared responsibility among the anesthesiologist, surgeon or proceduralist, and nurse in the operating room.3
- Common patient positions with their effects on hemodynamics, ventilation, and other physiologic factors are discussed below.
Supine Position
- The supine position is the most common position for surgical procedures with the patient lying on their back with the head, neck, and spine in a neutral position, and the arms either adducted alongside the patient or abducted to less than 90 degrees.1


Figure 1. Supine position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
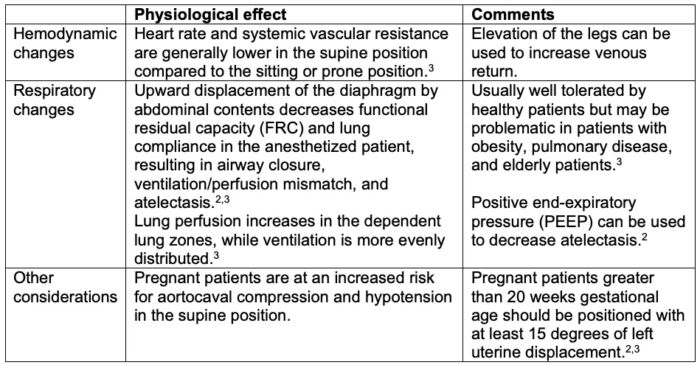
Table 1. Physiological effects of the supine position
Trendelenburg Position
- The Trendelenburg position is a variation of the supine position in which the head of the bed is titled down at least 15 degrees.2
- It is commonly used for intraabdominal pelvic surgeries, such as hysterectomy and prostatectomy. It is also used temporarily during central line placement.3 Steep Trendelenburg position is often used during robotic surgery.
- The Trendelenburg position has greater hemodynamic and respiratory effects than the supine position.3 (Table 2)

Figure 2. Trendelenburg position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
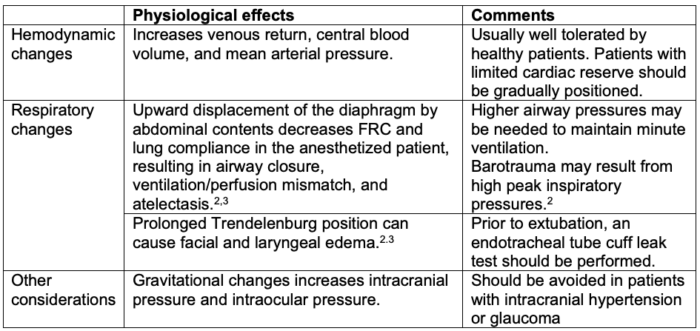
Table 2. Physiological effects of the Trendelenburg position
Reverse Trendelenburg Position
- The reverse Trendelenburg position is a variation of the supine position in which the head of the bed is titled upwards.
- It is commonly used for upper abdominal surgeries, such as cholecystectomy or gastric bypass to improve surgical exposure.

Figure 3. Reverse Trendelenburg position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
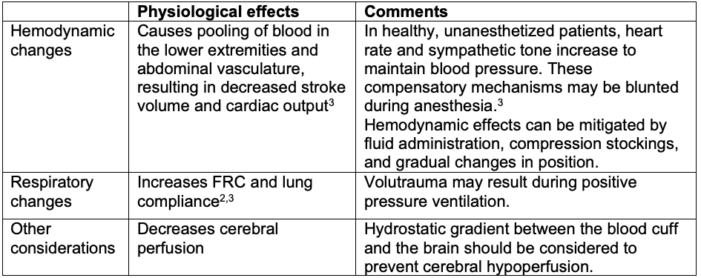
Table 3. Physiological effects of the reverse Trendelenburg position
Prone Position
- In the prone position, the patient is lying prone on their face and abdomen with head, neck, and spine in a neutral position, and the arms are either adducted alongside the patient or at a 90-degree angle at shoulders and elbows with palms facing down.1-3
- It is commonly used for spinal surgeries, posterior fossa craniotomies, rectal and buttock surgeries, and superficial back procedures.

Figure 4. Prone position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
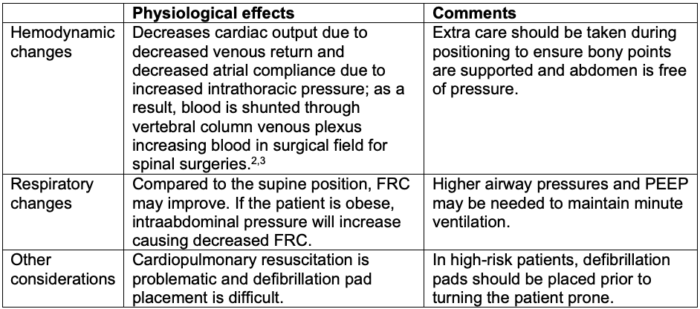
Table 4. Physiological effects of the prone position
Lateral Position
- In the lateral position, the patient is lying on their side with the operative side up. The legs are slightly flexed. The down arm is padded and the upper arm is supported on pillows or arm supports. A pad or roll should be placed under the chest wall to alleviate pressure on neurovascular structures in the axilla.2,3 Importantly, the roll should not be in the axilla.
- It is commonly used for hip, shoulder, and thoracic surgeries.

Figure 5. Lateral position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
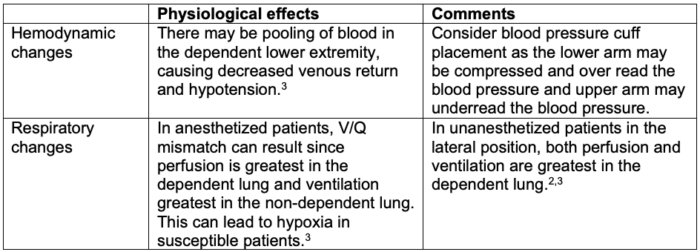
Table 5. Physiological effects of the lateral position
Lithotomy Position
- The lithotomy position is a variation of the supine position, with the legs separated and the hips and knees are flexed. The arms are either tucked in at sides or abducted on arm boards.
- It is commonly used for gynecologic, rectal, and urologic surgeries.

Figure 6. Lithotomy position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
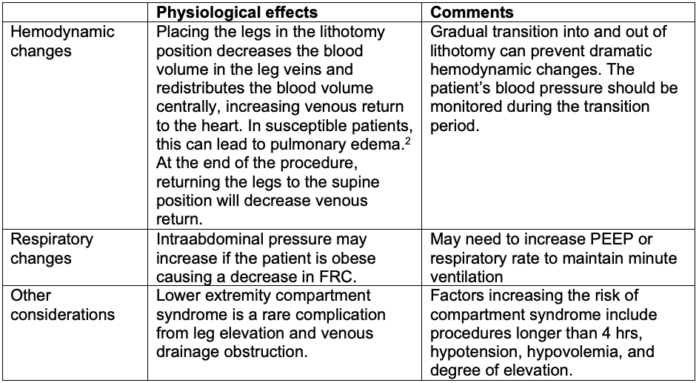
Table 6. Physiological effects of the lithotomy position
Sitting/Beach Chair Position
- In the sitting or beach-chair position, the patient is on their back, the head of the bed is raised, hips are flexed, and the legs are flexed at the knee.
- It is commonly used for shoulder and posterior fossa craniotomies.

Figure 7. Sitting/beach chair position (Illustration by Sarah St. Claire, RN, BSN, MS, CNOR)
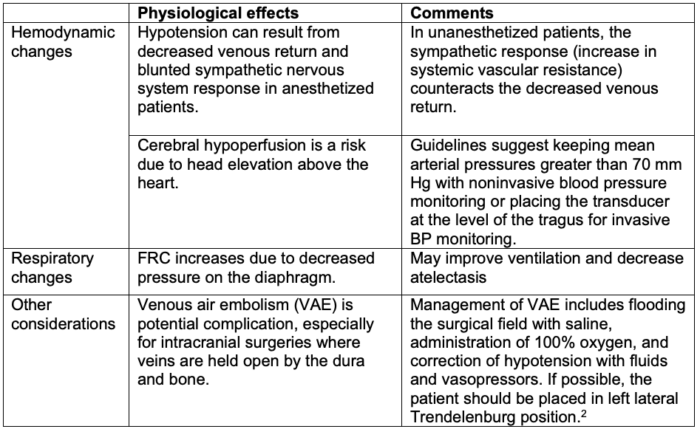
Table 7. Physiological effects of the sitting/beach chair position
References
- Armstrong M, Moore RA. Anatomy, Patient Positioning. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Link
- Hartley J, Baitch L. Patient positioning during anaesthesia. Anesthesia Tutorial of the week (ATOTW). 2015 World Federation of Societies of Anesthesiologists. Link
- Welch MB. Patient positioning for surgery and anesthesia in adults. In: Post T(ed). UpToDate. 2023. Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.